Overview
Targeted therapy is a newer type of cancer treatment that uses drugs or other substances to more precisely identify and attack certain types of cancer cells. Targeted drugs block the growth and spread of cancer by interfering with specific biochemical pathways in tumor cells that are important to their growth or survival. By targeting specific molecules involved in those pathways, the drugs can inhibit the growth of the tumor while limiting damage to normal cells. Targeted therapy is sometimes called “molecular targeted therapy” or “precision medicine”.
Targeted therapies differ from traditional chemotherapy in that targeted therapies try to alter how the cancer cells work. To do that, they focus on part of the cancer cell that makes it different from a healthy cell. In contrast, most standard chemotherapies kill rapidly dividing cancerous and normal cells. Like chemotherapy, targeted therapy drugs enter the bloodstream and reach most areas of the body, which makes them potentially useful against cancers that have spread. Because standard chemo is not very effective in most patients with liver cancer, doctors are focusing more on using targeted therapies.
Types of targeted therapy
There are many different types of targeted cancer drugs. They include both
- small molecule drugs that are are small enough to enter a cancer cell and target a specific substance inside the cell, and
- large molecule drugs that can’t fit inside a cell, but work by weakening or destroying proteins or enzymes on the cancer cell’s surface.
Most of these targeted therapy drugs work by one of the following mechanisms:
- Slowing or stopping the development of new blood vessels that feed the cancer cell (This type of drug is called an angiogenesis inhibitor)
- Blocking signals that tell a cancer cell to grow or divide
- Triggering the immune system to attack the cancer cell
- Changing specific proteins within a cancer cell, so the cell dies
- Carrying other types of treatments (like chemotherapy) directly to a cancer cell to kill it, while leaving normal cells alone (These are often called antibody-drug conjugates or ADCs).
Targeted therapies used in liver cancer and FLC
FLC patients are often treated with the following targeted therapies. All are approved treatments for HCC:
Protein kinases are enzymes on or near the surface of a cell that send growth signals. Kinase inhibitors and tyrosine kinase inhibitors are small molecules that block these chemical messengers. Blocking these proteins can often help stop a cell from growing and dividing and can slow the formation of new blood vessels. The growth factor receptors most commonly targeted by TKIs are vascular endothelial growth factor receptor (VEGFR), basic fibroblast growth factor receptor (bFGFR), platelet-derived growth factor receptor (PDGFR), and epidermal growth factor receptor (EGFR).
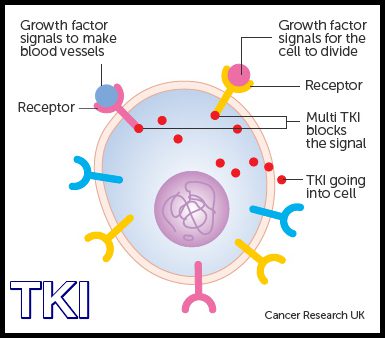
Source: Cancer Research UK
Specific kinase inhibitors that are currently being used to treat fibrolamellar include:
- Sorafenib (Nexavar) – a targeted therapy that blocks the growth of blood vessels and cancer cells. In 2007, sorafenib became the first targeted drug approved by the FDA to treat patients with HCC.
- Regorafenib (Stivarga) – blocks the growth of blood vessels and inhibits tumor growth. In 2017, regorafenib was approved as a treatment for HCC in patients who have already been treated with sorafenib.
- Lenvatinib (Lenvima) – another drug that blocks blood vessel growth. In 2018, lenvatinib was also approved to treat HCC.
- Cabozantinib (Cabometyx) – blocks blood vessel growth and some of the processes involved in tumor invasiveness and metastasis. In 2019, cabozantinib was approved for use in patients with HCC who have already been treated with sorafenib.
To try to overcome resistance, these targeted therapy drugs are frequently used in combination with other drugs, including:
- traditional chemotherapy drugs (e.g. GemOx plus lenvatinib; lenvatinib plus capecitabine), or
- immune checkpoint inhibitors (e.g. nivolumab plus lenvatinib).
Please see the discussion of combination therapies below and in the immunotherapy section.
mTOR is another type of kinase protein that causes cells to produce chemicals that trigger cell growth or initiate the development of new blood vessels. mTOR is involved in the control of cell growth and aging. By blocking mTOR, mTOR inhibitors can stop the growth of some types of cancer.
Monoclonal antibodies are man-made versions of immune system antibodies that attach to a specific target. They work by recognizing and finding specific proteins on cancer cells. Each MAB recognizes one particular protein. Depending on that protein, they can work in different ways to kill cancer cells or stop them from growing.
MABs that are sometimes used in fibrolamellar treatment include:
- Bevacizumab (Avastin) – a monoclonal antibody that targets vascular endothelial growth factor (VEGF), a protein that helps new blood vessels to form. This drug is currently used with the immunotherapy drug atezolizumab (Tecentriq) as the first treatment for HCC that cannot be treated by surgery or that has spread to other organs.
- Ramucirumab (Cyramza) – a monoclonal antibody that targets a VEGF receptor (VEGFR) protein on cells, which can help stop the formation of new blood vessels. This drug can be used to treat advanced liver cancer, typically after another treatment stops working.
Rationale for combination therapies
As with any systemic therapy, cancer cells can become resistant to targeted therapy drugs, causing the drugs to become ineffective over time. This resistance can occur if the tumor cells mutate so the drug no longer interacts well with the cell targets, or if the tumor finds a new pathway to grow that does not depend on the drug’s target. To help avoid this problem, targeted therapies are frequently delivered in combination with other drugs, rather than alone.

For many cancers like fibrolamellar, it is believed that combinations of drugs – a “one-two punch” of treatment – can achieve many benefits. Potential benefits include:
- Reducing tumor resistance to the treatment. By using drug combinations, the risk that a tumor is resistant to the drug decreases.
- Attacking multiple targets at once. The use of drug combinations allows doctors to target several factors driving a cancer’s growth simultaneously. Theoretically, working on multiple molecular targets at the same time should raise the chances of killing cancer cells and eliminating a tumor.
- Taking advantage of drug synergies. Sometimes a combination of drugs can be synergistic, meaning the impact of the combination is bigger than sum of the individual effects of each drug. For example, one drug could sensitize a tumor cell to another drug, making the combination much more effective than either drug alone.
However, combination therapies also have some risks or disadvantages, including:
- Increased side effects could be experienced because more than one drug is used
- The drugs could potentially interact in ways that cause additional new side effects.
Because patients with fibrolamellar carcinoma tend to be young and (aside from the cancer) usually have no underlying liver disease, many believe the benefits of drug combinations outweigh their risks. Consequently, there is a lot of activity, from early research to clinical trials, focused on investigating the use of different combination therapies in liver cancer and FLC.
Role of genomic profiling tests
Genomic profiling provides information about the specific genetic makeup of an individual patient’s cancer cells. To get this information, a sample of tumor tissue from a recent surgery or biopsy is analyzed to identify changes in the DNA (and sometimes the RNA) of the cancer cells. These tests generally do not perform a complete genomic analysis of the patient’s tissue. Instead they often look for specific mutations for which a drug treatment is already available, or under development.
For some patients, an “actionable target” is found. This means that the test discovered a particular mutation in a patient’s tumor that can be attacked by an existing drug.
Unlike many other cancers, FLC tumors tend to have few genetic mutations other than the DNAJB1–PRKACA fusion gene. As a result, many FLC patients do not receive actionable results from these tests. Nevertheless, many FLC patients opt to pursue the testing, hoping to find and potentially benefit from new emerging targeted cancer treatments.
Many major medical centers offer this type of testing to their patients. In addition, many commercial laboratories (including Caris, Foundation Medicine, Guardant, Molecular Health, and Paradigm) also offer tumor profiling tests. If interested, patients should speak with their medical teams about the costs and potential benefits of genomic or molecular testing.
Please note: The Fibrolamellar Cancer Foundation does not provide medical advice or recommend any specific organizations or services. We provide website users with information to help them better understand their health conditions and current approaches to the diagnosis and treatment of FLC. Always seek the advice of your physician or other qualified healthcare providers.