The following is a list of questions that patients and caregivers often have about fibrolamellar carcinoma, its treatment, and getting involved or finding support. Click or tap the box containing the question (or the arrow next to the question) to view the answer.
Many of these answers are from our own research and experience, and do not necessarily represent proven scientific fact. Please note that the Fibrolamellar Cancer Foundation does not recommend doctors, endorse specific organizations, give medical advice or promote any specific forms of treatment. Instead, we provide website users with information to help them better understand FLC and current approaches to diagnosing, treating and researching the disease.
Functions of the liver
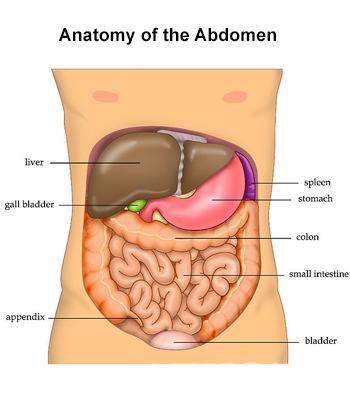
The liver is a large organ on the right side of the abdomen, above the stomach and below the lungs and diaphragm. It is protected by the rib cage. Adult livers generally weigh between 3 and 3 1/2 pounds and are reddish-brown in color. The liver is roughly triangular in shape and has two large sections: a larger right lobe and a smaller left lobe. The gallbladder, pancreas and intestines sit under the liver. The liver and these organs work together to digest, absorb, and process food.
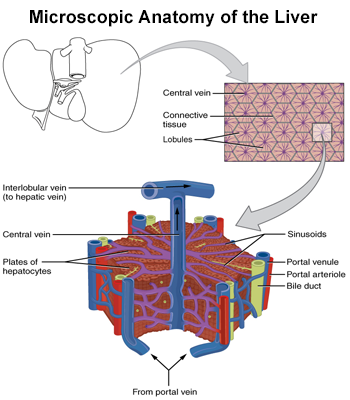
Unlike most organs, the liver has two major sources of blood. The portal vein brings in nutrient-rich blood from the gastrointestinal tract, and the hepatic artery carries oxygen-rich blood from the heart. The blood vessels branch into small capillaries, with each ending in a lobule.
The lobes of the liver are divided into roughly 100,000 liver lobules, where the vital functions of the liver are carried out. A typical lobule is 6 sided (hexagonal) and roughly 1mm in diameter. Each lobule consists of numerous cords of rectangular liver cells, called hepatocytes, that radiate from central veins toward the connective tissue that separates the different lobules. The plates of hepatocytes are one cell thick and separated by sinusoids, hepatic capillaries that give the hepatocytes direct access to the bloodstream.
The liver performs many essential functions. The liver is a vital component of the human digestive system, converting food into stored energy and chemicals necessary for life and growth. It removes waste products and foreign substances from the blood, regulates blood sugar levels, and creates many essential nutrients. It is impossible to live without the liver.
Overall, the liver performs over 500 vital functions in the human body, including:
- Eliminating the waste made after foods and other substances are broken down
- Producing bile, which carries away waste and breaks down fats in the small intestine during digestion
- Filtering blood coming from the digestive tract to remove toxins, byproducts, and other harmful substances
- Regulating blood clotting
- Producing albumin, the most common protein in blood serum that helps prevent fluids in the blood from leaking into other tissues
- Managing the conversion of fats from your diet and manufacturing triglycerides and cholesterol
- Converting carbohydrates into glycogen for energy storage and to make glucose as needed
- Regulating blood levels of amino acids, which form the building blocks of proteins
- Keeping the amount of nutrients in the blood supply at optimal levels
- Metabolizing bilirubin which is formed by the breakdown of hemoglobin and processing hemoglobin and storing its iron content for later use
- Converting poisonous ammonia to urea
- Storing certain vitamins and minerals, including vitamins A, D, E, K, and B12, for when they’re needed
- Helping to fight infection by making immune factors and removing bacteria from the bloodstream.
The liver is the only organ that can regenerate after it is damaged. If part of the liver is damaged or surgically removed, the remaining healthy liver can grow to compensate for the damaged or missing portion. Even if only 25 percent of the liver remains, regeneration can usually still happen.
FLC causes and impact
Treatment questions
Click here for a listing of doctors – including surgeons, oncologists and radiologists – who we know have treated patients with FLC. If physicians in your area are not listed, you can also contact one of the comprehensive cancer centers in the United States for additional names.

Because of the rarity of FLC and the lack of systematic studies of the effectiveness of specific treatments, no proven “standard of care” aside from surgery exists for the disease. While the specifics of how individual treatments are used depends on a patient’s situation and stage of disease, the main therapies for fibrolamellar carcinoma include:
- Surgery: Surgery is typically used to remove as much of the FLC tumor(s) as possible. This surgery can involve either a resection, where part of the liver is taken out, or a transplant, where the whole liver is taken out and replaced with a donor liver.
- Systemic treatments, such as chemotherapy, targeted therapy and immunotherapy: When surgery is not possible or when the cancer has spread, systemic treatments that can reach all parts of the body are generally used to treat FLC. Because of the lack of statistical evidence on which treatments are the most effective, doctors often select particular treatments based on drugs approved for use with HCC or by using their best judgement on a case-by-case basis.
- Ablation or embolization therapy: Depending on where the FLC tumor is positioned, embolization (cutting off a tumor’s blood supply) or ablation therapy (using temperature to heat or burn a tumor) can also be used.
- External beam radiation therapy: In cases where metastases have spread beyond the liver, radiation therapy is sometimes used to manage the progression of specific tumors.
Please see the treatment options section of this website for more information about these treatments and procedures. Alternatively, click here for an overview of treatments for FLC on Medscape.com.
When dealing with a complex medical condition like FLC, getting a second opinion can help patients feel more confident about their diagnosis and treatment plans. Doctors’ opinions can differ, and they can offer different treatment options based on their backgrounds and experiences. Some doctors take a more conservative approach to treating their patients, while other doctors are more aggressive and utilize the newest tests and therapies. As a result, pursuing a second opinion is a common practice for cancer patients.
There are many reasons why FLC patients may seek another opinion during the course of their care, including:
- to confirm their diagnosis
- to be certain there are no remaining options for surgery when the cancer is still confined to the liver
- to investigate treatment alternatives
- to increase their personal confidence on how best to proceed with their care.
Here are some tips when seeking a second opinion:
- Look for medical providers who have experience in FLC. This web site contains listings of doctor with FLC experience (see the find a doctor section on our site). Directly contacting major medical centers or other patients can also be a helpful source for finding experienced providers.
- Many physicians may review your case and consult over the phone, which can greatly simplify the process.
- Check with insurance providers to understand your coverage for second opinions and if a new specialist accepts your insurance.
- Plan to bring all medical records, including copies of exams, tests, previous treatments and scans to any appointments.
- Be clear about why you are seeking a second opinion. Do you want confirmation of a treatment plan? Are you looking to identify new treatment options? Discuss this at your appointment.
- Carefully consider what you plan to do next. Does your care need to be transferred to receive the new treatment options? Are you comfortable with the logistics of getting care somewhere else? Can a new treatment plan be communicated to your original doctor? When choosing to transfer care to another doctor, make sure that the change is communicated to your current medical team.
Patients’ decisions about their health care are critically important. Taking the time to understand and consider all treatment options and approaches is an important part of being an effective advocate for your health.
A clinical trial is a research study designed to assess the safety and effectiveness of a particular treatment, and advance the understanding of the science behind the cancer or the treatment.
Currently there are several clinical trials open to patients with FLC. They can potentially participate in clinical trials that are specifically for FLC, trials that are open to FLC patients, or studies that are open to patients with any solid tumor.
For more information on the latest clinical trials, view our clinical trials page, or visit clinicaltrials.gov and search for fibrolamellar.
Patients should ask their doctors about the availability and appropriateness of different trials. Potential clinical trials can also be identified using clinicaltrials.gov and the clinical trials page of FCF’s website. Within the detailed descriptions of each trial, contacts are listed who can be called or emailed to ask about the trial and to see if it is an appropriate option.
In addition to what patients can find out about the trial itself, other factors are also important to consider when selecting a trial, including where a trial is located, how frequently patients have to report to the trial site, the nature of the treatment, and the costs of participation.
Several sites give a good overview of considerations and questions to ask when choosing a study. These include:
- The American Cancer Society (click here)
- Clinicaltrials.gov (click here).
The preliminary results of on-going clinical studies are usually not publicly available. For phase 2 or 3 trials, there may be published reports on the results from earlier phases. Occasionally, case studies of a trial treatment in a few patients may be published as well. If available, patients can sometimes find this information by performing an internet or literature search using the name of the drugs, the company and the condition treated.
However, as with all treatments, there is no way to predict what the results will be for a particular patient.
Genomic testing, also called molecular profiling or genomic profiling, looks for gene mutations within a tumor known to be associated with cancer. These are relatively new tests and they do not always provide patients with useful results. However, because there are many existing and emerging cancer treatments that target specific genomic mutations (see targeted therapies in the treatment options page), this testing can sometimes allow doctors to recommend treatments that target specific mutations within a patient’s cancer, or treatments that they feel could be effective based on the total tumor mutation burden (a measurement of the number of mutations carried by tumor cells).
Many major cancer centers, including Dana-Farber, Memorial Sloan Kettering, Mass General Hospital, University of Washington Medicine and others, can conduct a genomic analysis for patients. Some medical centers now routinely perform genomic tests for all cancer patients. In addition, several private companies, including Caris, Foundation Medicine, Guardant, Molecular Health, and Paradigm, perform their own versions of genomic testing.
Unlike many other cancers, FLC tumors often have relatively few tumor mutations other than the DNAJB1–PRKACA fusion gene. As a result, many FLC patients do not receive actionable results from these tests. Nevertheless, many FLC patients opt to pursue the testing, hoping to find and potentially benefit from new emerging targeted cancer treatments. If interested, patients should speak with their medical teams about the costs and benefits of genomic or molecular testing.
It is believed that most cases of FLC occur at random and not as a result of an inherited genetic trait. The fusion gene that is specific to FLC is a somatic mutation and not a germ-line mutation, an inherited genetic alteration that occur in sperm and eggs. Unlike germ-line mutations, which can be passed on to descendants, somatic mutations are not usually inherited. Somatic mutations are frequently caused by environmental factors, such as exposure to certain chemicals.
There is, however, a rare, inheritable genetic condition called the “Carney complex” that is characterized by spotty skin pigmentation and heart myxomas (a type of tumor). A few fibrolamellar carcinomas have been identified as part of the Carney complex. However, these fibrolamellar carcinomas have a mutation in the PRKAR1A gene instead of the DNAJB1-PRKACA fusion gene found in most fibrolamellar carcinomas.
Each patient’s doctor should determine which is the best scan to use and at what time intervals. Different scans yield different information and expose patients to varying amounts of radiation. CT scans do expose patients to additional radiation and in certain circumstances your doctor may choose to use a MRI, which is a form of imaging that uses magnetism and radio waves instead of radiation.
Studies have shown that there is a very small risk of developing a second cancer as a result of treatment with radiation or some types of chemotherapy. If a patient is concerned about these risks, it’s important for them to discuss their concerns with their treatment team. Doctors generally believe that the benefits of cancer treatments, including external beam radiation therapy, vastly outweigh these risks.
Doctors do not generally recommend specific diets or lifestyles for FLC patients. However, for most patients, it is important to eat a healthy diet and stay in good physical shape. The healthier a patient is entering treatment, the greater their chances of a smooth recovery. Patients should consult with their doctors about any restrictions in activities or diet that may be important to their health.
Getting involved or finding support
Please note: The Fibrolamellar Cancer Foundation does not provide medical advice or recommend any specific organizations or services. We provide website users with information to help them better understand their health conditions and current approaches to the diagnosis and treatment of FLC. Always seek the advice of your physician or other qualified healthcare provider.