Overview
A common treatment for fibrolamellar carcinoma (FLC) is surgical removal (resection) of the tumor. Doctors sometimes use the term resectable to describe cancers they believe can be removed by surgery and unresectable to describe those they think are too difficult to be entirely removed by surgery. Surgical treatments for FLC include both curative surgery and palliative surgery. Curative surgery removes all visible traces of cancer from the body. Palliative surgery means the goal is to “debulk” the tumor, improve symptoms, lessen pain or provide better quality of life, even when all visible tumor can’t be removed.
Surgery is the only treatment for FLC that is proven to be potentially curative. As a result, many patients will go to great lengths to make sure surgery is a viable option for their treatment, including:
- consulting with multiple surgeons about whether or not their disease can be completely resected
- working with their surgical and oncology teams to identify systemic treatments or interventional radiology treatments that could potentially shrink the disease enough to make them a candidate for surgery.
Because the liver is the only organ which can regenerate itself, it can grow to compensate for the removed portions after surgery. This can allow surgeons to resect up to 70-80% of the liver in exceptional cases. After liver surgery, liver function typically returns to normal within 2 to 3 weeks of resection surgery and liver size returns to normal within 3 to 6 months.
Surgical approaches for FLC
Two main types of surgery are used to treat FLC that has not spread beyond the liver. These include:
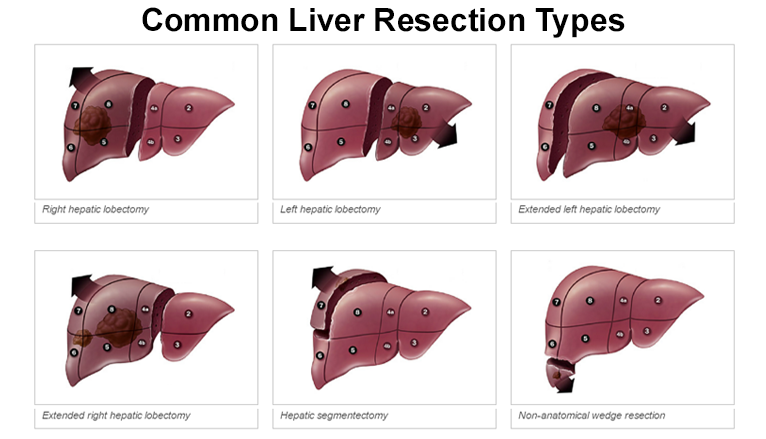
Liver resection is the surgical removal of a portion of the liver. A wedge resection (also called a segmentectomy) involves removing the area of the liver where the tumor is located; a lobectomy involves removing the whole lobe (section) of the liver that contains the tumor(s). Both are complicated operations and require an experienced team of surgeons and assistants. If the amount of liver tissue removed is not too great, the liver will function normally because its tissue has the ability to grow back.
If a patient is a candidate for surgery, their surgeon will likely discuss resection margins when planning treatment. Because tumor cells left behind after surgery can potentially re-grow, removing both the tumor and wide margins of healthy tissue surrounding it will lower the risk of the tumor coming back after surgery. A wide resection margin is the best outcome, if possible. However, the location of tumors near important structures like critical blood vessels sometimes makes wide resection margins impossible to achieve.
In some cases, a patient’s medical team may prescribe a course of chemotherapy or other systemic therapy before surgery in order to shrink the tumor to make it easier to remove. In addition, some doctors prescribe chemotherapy after surgery to reduce the chances of stray tumor cells causing a recurrence of the disease.
After liver resection surgery, most patients can expect to be in the hospital anywhere from five to seven days, depending on their prior health and the size of the incision. Patients generally should be out of bed the day after surgery, and able to eat a limited diet and walk before they are discharged. Patients that are still in pain at discharge will be given a prescription for pain medication. Doctors generally advise that recovering resection patients slowly increase the amount of walking they do and perform regular, moderate tasks every day to help with leg swelling and fatigue. However, patients should avoid lifting anything over five pounds for eight weeks, and need to wait for a doctor’s go-ahead before safely driving a car.
Total hepatectomy (removal of the entire liver) followed by a liver transplant is possible when cancer has not metastasized, or spread beyond the liver. This surgery offers a high survival rate, but it is a more involved surgery that can take up to 12 hours and requires a long recuperation time.
Traditionally, patients needing a liver transplant had to wait until a suitable liver from a recently deceased person became available. In recent years, doctors have been able to successfully transplant a portion of a liver taken from a healthy living donor. (The donor’s liver will regenerate, or grow back, over time.) The donor must go through an evaluation to be sure his/her liver is healthy and suitable, but he/she does not need to be a family member of the recipient. Living donor liver transplantation has the benefit of increasing the availability of organs, and transplants can be scheduled in advance. However, the majority of liver transplants are still from deceased donors.
Patients with fibrolamellar who are awaiting a liver transplant from a deceased donor will be put on a “waiting list” managed by UNOS, the United Network for Organ Sharing. Priority on the UNOS list depends on a patient’s MELD score (model of end stage liver disease), with the sickest patients moving to the top of the list.
There are many requirements for liver transplant surgery, many of which are specified by the patient’s surgical hospital of choice. In general, before a patient can begin the liver transplant evaluation process, they must be free of:
- Cancer outside the liver
- Substance abuse
- Active infections
- Disabling psychiatric conditions
- A documented history of not following medical instructions
- Other diseases or conditions.
Most institutions also want to be sure that the patient is willing and able to make the lifestyle changes to support the gift of life that a liver transplant provides.
After a liver transplant, most patients are able to resume normal daily activities after a couple of months, although full recuperation can take as long as six months. Transplant patients also need to take anti-rejection medication for the rest of their lives. Since the anti-rejection medication weakens the immune system, they may need to take additional medications to prevent infections as well.
In addition, although a transplant can be potentially curative, it could prevent a patient from trying new immunotherapy treatments in the future. Because of the increased risk of organ rejection after a transplant, immunotherapy may not be an option if a transplant patient experiences a recurrence of the disease.
For more details on liver transplants, see https://www.mayoclinic.org/tests-procedures/liver-transplant/about/pac-20384842
For more details on living donor transplants, see
https://my.clevelandclinic.org/health/treatments/21083-living-donor-liver-transplant
Tumor recurrence
It is possible for tumors to recur (return) even when resection and/or transplantation has been considered successful. Different studies have shown that between 43 percent and 65 percent of all patients with liver tumors (including, but not exclusive to those with fibrolamellar) have recurrences within two years of a liver resection.
For that reason, patients are typically monitored with regular checkups and CT and/or MRI scans at regular intervals to watch for signs of recurrence. Most recurring tumors tend to appear within a few years of surgery, but patients are typically monitored for 10 years or more to be on the safe side. Depending on where they show up, recurring tumors are frequently treated with another surgery.
Please note: The Fibrolamellar Cancer Foundation does not provide medical advice or recommend any specific organizations or services. We provide website users with information to help them better understand their health conditions and current approaches to the diagnosis and treatment of FLC. Always seek the advice of your physician or other qualified healthcare providers.